Methicillin-Resistant Staphylococus Aureus
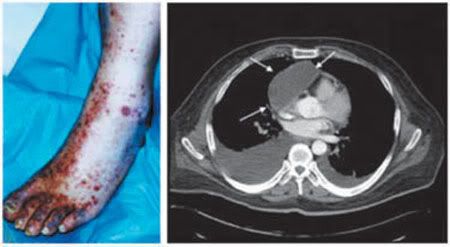
Taken from Mayo Clinic Proceedings, showing an external and internal S. aureus infection.
This is the second time I'm hitting on this subject, the last time was in Why Are We So Bent Over Bird Flu? where I wondered why it is we're so excited about bird flu, which even now has killed less than a couple of hundred folks world wide, yet so sanguine, apparently, about MRSA, the acronym for the title to this blog. In the Nov 3 issue of The Economist, specifically in MRSA : The struggle against superbugs we're informed about MSRA and that it kills about 90,000 Americans a year. This week you can read in U.S. News & World Report another article, Bugs behaving Badly: Antibiotics are aging, and bacteria are learning to fight them off about very much the same thing, in fact the 90,000 fatalities number is also given. U.S. News takes it a step further by telling us that it's more than Staph. a. that we need to be concerned about, indeed we can add to the list clostridium difficile, acinetobacter baumannii, and neisseria gonorrhoeae. These were all bacteria that were very treatable with general antibiotics in the past and are now resistant and, obviously, life threatening; the list is only going to grow. So in short, with S. aureus if it doesn't kill you it can do a serious number on your body and the list of deadly bacterial companions continues to grow (additional information specifically regarding MRSA can be obtained from Kent County Health Dept. Fact Sheet.)
With Stap. A. we have a bug that not only can kill you, and does so to the tune of 90,000 folks a year, but can disfigure as well, and there's no national program to address this issue, no major ruckus by our politicians to fund a program to educate the public and to provide incentives to drug companies to make it worth their time and money to actually focus on new antibiotics that could get ahead of drug resistant strains of common bacteria. Just as a reminder, S. aureus is quite common, having a preference for hanging out in mucous membranes so it's fairly commonly found in the nose, and even on our skin.
There are a few things that can be done to help ameliorate if not solve this problem:
1. As far as things to be done are concerned, what should top the list is the government providing monetary incentives to drug companies to come up with new antibiotics. It's not as if we can't come up with them, i.e. the bugs aren't getting beyond antibiotics in general, but rather that there's little money to be made in antibiotics and in turn few drug companies put much effort into them. So throwing some incentives at drug companies for new antibiotics and new strategies to fight these bugs would indeed be a public health service worthy of just about as much money as we're throwing at bird flu, or about a week's worth of occupation in Iraq. When the government looks to spends hundreds of millions on bird flu vaccines they're throwing money at drug companies to induce them to produce an equally low-profit item, doing so for MSRA and antibiotic resistance in general would be a definite public service.
2. Doctors need to stop over-prescribing antibiotics. I appreciate that a parent with a child that's screaming its head off from a viral infection wants something to fix the problem, but we all know (ok, we don't all know ...) that antibiotics don't work on viral infections and otherwise help to build up antibiotic resistance in the bugs that inhabit our body. Doctors more and more don't have the time to tell their patients this so it's easier to prescribe an antibiotic and be done with it, but this definitely fuels the problem and it needs to stop. A patient screaming for percodan shouldn't get them, why should someone screaming for antibiotics? Well, the fact is the doctor doesn't go to jail for over-prescribing antibiotics ...
3. Doctors and hospitals need to be clean freaks. In Denmark, Finland, and the Netherlands the incidence of MRSA infections are much lower than in other countries, and the main difference seems to be cleanliness protocols. Doctors need to wash their hands before, after, and in between every patient, but really, who wants to be bothered with that with so little time?
Hospitals need to be scrupulously clean, but with HMOs looking for those cost saving measures where do you find the staff to keep things clean? Well we have to figure out how to up the priority on this as the number of people dying from resistant bugs bred in hospital environments such that it's hard to picture any possible justified cost-savings in not doing so, though cost-cutting mentalities are all too often stovepiped such that they don't see the potential harm done by being too niggardly when it comes to cleaning supplies.
4. Antibiotics are used in huge numbers in the livestock industry for a couple of reasons. First, and the one the industry will most often give as a reason, is to reduce infections in the livestock population. Now of course this flies in the face of the prophylactic use of antibiotics with humans where it's been found that the only thing it does is eventually build up a resistant strain of the bugs you're trying to avoid. Second, and the main reason antibiotics in animal feed is so attractive, is that for reasons I'm not clear on, I'm not sure anyone is, livestock bulk up on antibiotics up to 10%, so of course that cow in the feedlot is now worth 10% more if it has some antibiotic munchies in its corn feed. So we're fattening our cattle and helping to create antibiotic resistant strains of bugs that the cattle live with, and somehow that's supposed to be good us ... oh boy.
5. People in general, to include people who certainly should know better, need to understand and appreciate the difference between viral and bacterial infections. Of course I understand much this may be to expect for a country where so many have a hard time with evolution much less understanding the difference between viruses and bacteria, but we really need to try. The U.S. News article cited above has some a good article attached to it entitled Want to help? Just say "Whoa" which provides some good information on how not to abuse antibiotics and a number of good links, to include: 1. an animation from the U.S. FDA center for veterinary medicine explaining how bacteria becomes resistant (Animation of Antimicrobial Resistance), 2. some info from the CDC's Get Smart campaign, Spotlight: Snort. Sniffle. Sneeze. No Antibiotics, Please!, and finally we have 3. Tuft University's APUA: Alliance for the Prudent Use of Antibiotics which provides information for consumers & patients, healthcare providers, and researchers, as well as information on antibiotics in the ecology and the international problem with antibiotics.
Lastly, it always helps if you raise a stink with your local national representatives, by letter if possible (they tend to take letters a bit more seriously than simply emails, and they take calls even more seriously), to let them know that you think this is an issue you think the federal government should be doing more about. I'm not a believer in the government, any government having all the answers. But right now throwing some hundreds of millions of dollars at bird flu when we already have a catastrophe (really, how else would you describe 90,000 people dying from something every year?) running rampant through this country, is a ridiculous focus of resources (I won't even get into the war in Iraq) and does more to endanger Americans in the long term than just about anything else you can point a finger at.
posted by James at 3:59 PM
![]()


12 Comments:
My pediatrician always trots me out for her new nurses and med students with the following explanation: "Here is a GOOD parent who doesn't demand antibiotics at the first sniffle." I guess you could say that parents today are overworked and incapable of dealing with a sick kid for longer than 15 minutes, and their indoctrination makes them demand SOMETHING when they've gone to all the trouble to penetrate the fifteen levels of gatekeepers it takes to actually get an appointment to see a doctor. People expect that modern medicine should have an answer for everything short of cancer.
As the the use of anitbiotics in our meat industry, this is absolutely something which is overlooked. My kids rarely get sick, but I've noticed a marked uptick when I started getting the healthiest meat and milk I could for them to consume.
I also used to have a neighbor who would bundle her kids in three layers of clothing whenever the temperature dipped below 75 degrees. My little redneck chirren ran around barefoot until it was practically freezing in a t-shirt and shorts. Guess whose kids were by far the sickest?
The bird flu has captured the imagination, but it is the need to be on guard against the illnesses you describe that is the most pressing. Unfortunately, we haven't put our mind toward "encouraging" pharma companies to come up with new answer, nor do your average people understand the difference between a virus and a bacterium.
Ms. Cornelius,
We're expecting our first child in about two months and you just gave me something to chew on that I hadn't really thought about - what will we be feeding her? I'm sure my wife and I will be giving this a lot more thought.
Your experience with letting your children out with little clothing may not exactly match up with something I remember watching (I think it was part of the PBS series, "Evolution" now that I thin about it), but it bears mentioning. What kids would one expect to be healthier: City kids or those on farms? I suppose for some it may be a hard call, but for anyone with some understanding of the process it comes as little surprise that the farm kids, who are constantly exposed to bacteria and what not (I'm not sure exactly what "What not" would constitute, but I'm sure you get the idea) are healthier, have fewer infections and debilitating encounters with germs. There's something to be said for throwing one's self, if not one's children, into the muck in an intelligent way.
As for virus vs. bacteria, you're right, and it amazes me how something so fundamental should be beyond the understanding of the average person given what either of these two are responsible for.
Congratulations, James! --And get some sleep while you can. I wish you all the best of health.
Atmikha
Atmikha,
Wow, for some reason I thought you knew about this ... how odd, but I guess this happens in the cyberworld we inhabit. And, of course, thanks from me and the Mrs. for the congratulations!
You're right, we're going to have to do our best to get sleep. Fortunately my mother-in-law will be coming in from Iran to stay with us for about six months to help out, so hopefully sleep deprivation won't be too terrible!
Maybe I did know and I forgot. They say Alzheimers starts in your 30's.
It's still great news! -- And I'm just as happy for you and Feri all over again. You guys will be great parents.
Atmikha
Congratulations, James!
I'm a mom-- I've got loads of advice that no one in my house listens to! Feel free to ask! Please, it would make my day!
And it was bit of joking about the freezing temperatures part, but really, the guideline is, check to see if their little fingers, toes, nosetips are cold. If not, the baby doesn't need more clothes on. We build immunity through being judiciously exposed to things not from wrapping up in cotton batting.
Now about that nipple confusion thing.....;-)
This sequence really "covers the waterfron". As a somewhat senior "senior citizen" I have several comments. the overprescribing of antibiotics is not new. I remember worrying about this 50+ years ago when the knee-jerk reaction was to prescribe an antibiotic. There was even an abomination calld Achrocidin that contained Achromycin, an antihistamine and an antipyretic/analgesic that was marketed specifically for the treatment of the common cold. My impression is that such foolishness has continued unabated-simply in a different form.
With respect to energizing the immune system, my granma used to say,"a child must eat a pound of dirt to grow up healthy". But Dr. Henry Smyth of the U of PA med school developed the toxicological concept of "adequate challenge" that, in fact said the same thing my grandma said, I have always contended, to no avail, that toxicology testing should be done on Norway rats collected on the San Francisco waterfront rather than on white rats mollycoddled for countless generations in aseptic conditions.
And finally, and most frighteningly, Baptiste et al-Emerg Infect Dis 11(12) 2005 have recently shown that MRSA can be transmitted from dogs to humans!!
wish to post my observances of hygiene at one modern hospital-- Following a minor day-surgery requiring an anaesthetic, my spouse arrived beside my bed to drive me home.. I was aghast to note his dirty work clothes and shoes which i knew he wore the previous day around farm animals (we lived in a rural area). The 2-bed ward was carpeted!!! Also the almost constant presence of visitors' children using everything including the en-suite toilet facilities is not to my mind strict hygeine.. Also, the former 'starchy ward sister' has vanished. I noted a nurse (I think she was a nurse?)took my blood stained dressings in her bare hands to the ensuite area.. In previous times, they would have been carried in a covered dish taken to a disposal area. Another issue re the hospital germ spread is the failure to cover patients' feet prior to entering the operating theatre. In previous times this was done.. no-one checked if my bare feet had fungal infections or clean after walking around the carpeted ward. In another hospital a patient took bets with the next bed patient re how long it would take for a sweet wrapper to be removed from under another bed-- it took 3 days-- a far cry from the old daily polished linoleum flooring scenario! Re the antibiotic use, it would be helpful if doctors could take a little more time where necessary, in evaluating virus versus bacterial situations, which in some cases, could reduce more intensive antbiotic use (and other services) for initially un-recognised serious bacterial infection. I believe modern hospital hygiene and time factors contribute to the woeful staph situation.
Anonymous from last night: Your observations certainly fit with is being reported and what those of us who should have some clue about the difference between viruses and bacteria see all the time - the fact is that citizens are woefully under-educated and caring, which to a large degree leads to the abuse of these drugs. I am certainly not surprised by inter-species transfer of MSRA or anything else, and this whole thing is likely to get worse before it gets better.
Anonymous from this evening: Your account of your hospital stay is, to say the least, chilling. It's clear based on the fact that certain European countries have much lower incidences with MSRA that a large part of the problem is the cleanliness oversight, or lack thereof that comes with today's hospitals. With everything having to be "cost-effective" cleanliness falls by the wayside, resulting in all the things that you noticed while in the hospital. In addition there's a real problem with staffing of hospitals, especially with there being nurses. So what nurses may have done in the past isn't getting done for lack of the bodies to do it, and those who are there are often over-worked or, I'm sure, insufficiently aware of the negative repercussions of their negligent cleanliness habits.
Atmika: I'm sure you're hardly suffering from Alzheimers. I sometimes think I've said something to friends when in fact I merely posted it online in the blog and it's hardly reasoanble to expect that friends will see everything that makes it there. Anyway, thanks for the congrats! I also hope we're able to make the "parental" grade as it were, but given some of the examples I've encountered as a teacher thus far I'd have to say that making at least a "C" wouldn't be a huge problem.
Ms. Cornelius: Thanks for the offer of advice, I'll likely take you up on it as both Feri and I have little clue as to what we're getting outselves into. Ok, we've done some reading, and the fact is that before she became a neuro-physiologist Feri was a mid-wife who delivered some 200 babies, but on the whole we're both newbies.
As for the nipple confusion thing ... with the mom-in-law on hand, a veteran of five of her own, I'm pretty sure we'll figure things out, though I'm pretty sure there'll be more than a few interesting stories to come from it!
Nice post, but the 90,000 figure is for all hospital-acquired infections, not just staph. And yes, you should worry about Acinetobacter.
Mike, You're right regarding the 90K from all infections, not just staph. Somehow I managed to mix staph in with everything, but my understanding is that MSRA isn't just staph but includes any bug that would acquire antibiotic resistance. However we cut it, any bug that we might be concerned about that has in the past been susceptible to being treated with antibiotics is rapidly moving into the category of a superbug that will resist any antibiotic treatment - in some cases it may not be a rapid movement into so much as it's already there.
Thanks for the clarification!
Post a Comment
<< Home